Partial Transcript
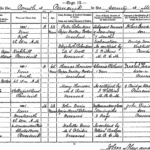
| No. | Name and Surname. | Rank or Profession, and whether Single, Married, or Widowed. | When and Where Died. | Sex. | Age. | Name, Surname, and Rank or Profession of Father. | Name, and Maiden Surname of Mother. | Cause of Death, Duration of Disease, and Medical Attendant by whom certified. | Signature & Qualification of Informant, and Residence, if out of the House in which the Death occurred. | When and where Registered, and Signature of Registrar. |
|---|---|---|---|---|---|---|---|---|---|---|
| 36 | John | Joiner | 1891 June Fourteenth 8h 50m AM | M | 43 Years | John Durie | Isabella Durie | Inflammation of Ear Meningitis 3 Days |
John Durie | 1891 June 15th |
| Durie | Married to Jane Tear | 6 Manderston Place, Shottstown, Penicuik | Agricultural Labourer Deceased |
MS Blaikie Deceased |
As certified by William Badger MBCM | Son (Present) |
At Penicuik [Signature] |